
Table of Contents
What is a HeRO graft?
- A HeRO graft also sometimes referred to as a HeRO catheter is an arterial to venous graft which allows high flow of blood for dialysis. Hero grafts are generally used in patients who have few options for venous access for dialysis.
- If venous outflow tracts are stenosed or narrowed because of prior raft and dialysis catheter placement patients may undergo venoplasty to allow for positioning of the venous component of the graft.
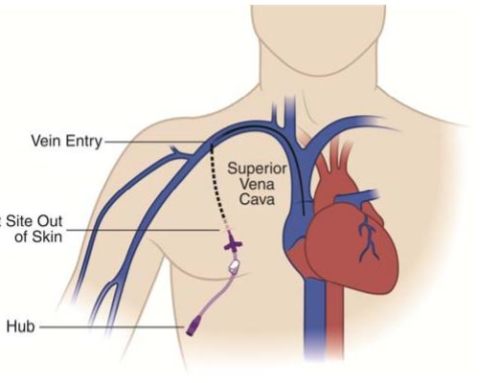
- Hero grafts have an arterial component that attaches to an artery usually on the upper arm. it is then connected to the venous outflow component which has a tip in the veins near the right atrium of the heart. The arterial component and the venous outflow components are connected using a titanium connector which is responsible for attaching the arterial graft component to the venous outflow component.
- Venous outflow component is made of silicon with marker bands at the distal tip to allow for better visualization and positioning in the right atrium. This venous component is inserted in to the internal jugular vein and it advances up into the right atrium. This can be done under ultrasound guidance with fluroscopy to confirm the positioning of the tip of the venous component.
HeRO Graft placement
The placement of hero graft is similar to that of a hemodialysis catheter combined with a graft.
The 90 minute procedure is done under general anesthesia. The central venous outflow component is placed in the central vein using the percutaneous endovascular techniques. This way, the tip is somewhere in mid to upper right atrium.
The titanium connector joins both the components such that the arterial graft lies at the deltopectoral groove. An arterial anastomosis joins the arterial graft to the target artery.
Advantages of HeRO Graft vs Fistula
- Reduction in the incidence of infections by 69 percent as compared to dialysis catheter
- Superior dialysis adequacy with 16% to 32% improved dialysis clearance of toxins and fluids when compared with dialysis catheters
- Patency rates which are significantly better than dialysis catheters and similar to arterio-venous grafts. The reported patency rates are up to 87% at 2 years
- These grafts are thought to be cost saving with a 23% average savings per year compared with dialysis catheter placement and management.
How is a HeRO Graft Accessed for dialysis?
• A light tourniquet may be used to dilate the graft.
• If cannulating toward the arterial anastomosis incision, stay at least the length of the fistula needle from the incision site.
• NEVER cannulate the Venous Outflow Component.
• Cannulate 3” (8 cm) from the Connector incision site to avoid damage to the graft rings.


Leave a Reply