
Laceration of a hepatic artery resulting in extravasation of contrast

Angiogram and ultrasound of a hepatic artery pseudoaneurysm

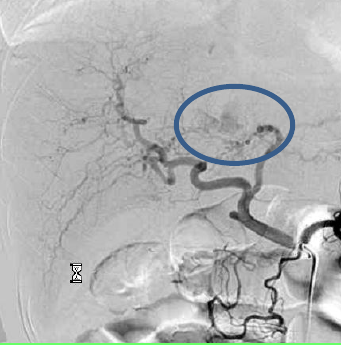
The image represents a GDA (gastroduodenal) Pseudoaneurysm secondary to pancreatitis.

CT and Angiography of a splenic artery aneurysm
Splenic artery aneurysms are the most common visceral artery aneurysm, accounting for 60%
Treat is generally recommended if > 2 cm.
Treatment options: (1) coil if saccular, (2) coil front & back door if irregular or wide mouthed, (3) covered stent if fusiform.
∙ Causes of visceral artery trauma include the following: Pancreatitis, PUD, pancreatic CA, trauma, iatrogenic (liver biopsy, etc)
∙ Treatment: Exclude pseudoaneurysms either by “trapping” and in essence embolizing it with coils on either side or by directly packing coils inside of it or by placing a covered stent across the injured vessel. Alternatively some pseudoaneurysms such as may occur in the groin involving the common femoral artery (from prior angiography) can be treated by compression or thrombin injection under direct ultrasound guidance to induce thrombosis.
For active extravasation/active bleeding, selective microcoil embolization is preferred, but gelfoam can also be used but is a less permanent solution and has a role in certain situations. ∙ If you embolize something through the SMA, you must follow with a celiac angiogram to ensure no additional supply to pseudoaneurysm as the vascular supply in this area is redundant. And vice versa.
SUMMARY:
●Although aneurysmal degeneration of visceral vessels is rare, visceral artery aneurysms (VAAs) are detected more often than in the past due to the increased use of cross-sectional body imaging and ultrasonography. True visceral artery aneurysms involve all layers of the wall, each of which is thinned but intact. Visceral artery pseudoaneurysms (VAPAs) result from a tear in the vessel wall due to trauma (iatrogenic, blunt, or penetrating injury) with subsequent periarterial hematoma formation.
●The splenic artery (VAA) and hepatic artery (VAPA) are most commonly involved. Less commonly involved are the celiac and mesenteric arteries, and gastric, intestinal, pancreatic, gastroduodenal, pancreaticoduodenal, and inferior mesenteric artery aneurysms are much less frequently reported.
●Visceral artery aneurysms are usually asymptomatic and identified as incidental, unexpected findings on imaging of the abdomen, particularly on computed tomography (CT) of the abdomen or CT angiography.
●The pathogenesis of VAA is poorly characterized as VAAs may be associated with a variety of conditions, including atherosclerosis, medial degeneration, and conditions of increased flow (eg, pregnancy, portal hypertension, liver transplantation). The natural history for VAA located in different anatomic locations is not uniform and also not well defined.
●The clinical presentation of symptomatic VAAs differs for each anatomic location; however, clinical symptoms and signs are nonspecific, and VAA and VAPA are often not suspected initially in patients presenting with abdominal complaints, due to their rarity, which can lead to a delay in diagnosis. For patients in whom the diagnosis is suspected (eg, pregnant women with sudden left upper quadrant pain), imaging demonstrating the aneurysm is required to confirm the diagnosis. For patients presenting with rupture, the diagnosis may necessarily be made in the operating room.
●The general approach to VAA/VAPA is early elective intervention, rather than watchful waiting, to minimize the risk of rupture. Observation with surveillance is an option for some small aneurysms in those who are poor risk for intervention, or who have a limited life expectancy.
●Treatment is indicated for:
•Any VAPA, when identified (symptomatic or asymptomatic)
•Symptomatic VAA
•Asymptomatic VAA that:
–Has a diameter more than 2 cm
–Expands more than 0.5 cm/year during observation
–Occurs in a woman who is pregnant
–Occurs in a woman of childbearing years
–Occurs in a patient undergoing orthotopic liver transplantation

